If we summarize these symptomatologies, it follows that posture disorders in infants can have as their origins:
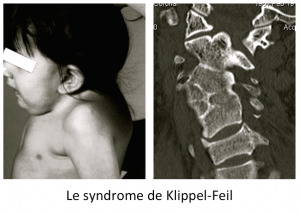
- An articular malformation,
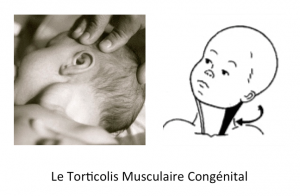
- Muscular hypertonicity,
- A neurological condition,
- A digestive origin,
However, it is never mentioned that the child can simply have a dysfunction of the articular mobility of a vertebral stage.
It is possible and it is what we call KiSS syndrome.
In fact, KiSS is a blockage of the cranio-cervical junction, i. e. the first joint between the base of the skull and the first cervical vertebra.
This joint dysfunction results in a postural adaptation of the whole body.
In keeping with the osteopathic concept, Sutherland used the following metaphor when referring to an Anglo-Saxon saying:” As the twig is bent, so is the tree inclined ” which could be translated as : ” As the young shoot is curved, the tree bends “[2]. We then understand the interest of early osteopathic management of these children.
CO/C1 subluxation, hypothesis explaining the adaptive mechanisms of KiSS
In this case, the head is rotated right and tilted left.
Ligaments and muscles in the suboccipital region are under stress, resulting in muscle spasm.
The cranio-cervical junction is impacted.
When the skull is dysfunctional, the centre of gravity is changed. There will be negative effects on the neurological and vascular structures of the base of the skull and neck. In particular, structures near the musculature will be under stress.
The vertebral arteries and first cervical nerves protrude from the posterior part of the occipito-atlantoid ligament. It is very likely that this ligament and others cause irritation of the neuromuscular system in KiSS syndrome.
Similarly, suboccipital ligaments, spinal erector muscles, small and large oblique, sternocleidomastoid, scapula elevators, trapezius, scalenes (especially anterior scalens) are involved in this situation.
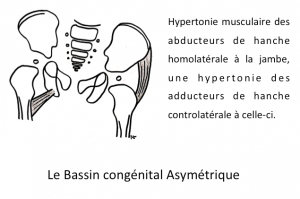
Through the inclination of the skull, and the tensions of the muscles of the cervical spine, the pelvis will be positioned on one side to compensate for the imbalance of the body.
The pelvis pulling on one side of the spine will tilt the spine, causing a contraction of the back muscles on one side, and creating the opisthotonos.
False hip subluxation may be the result.
The corrective technique of KiSS syndrome leads to a normalization of C0/C1 subluxation. This also harmonizes the adaptive phenomena seen above.
The reharmonization process, after the correction of the C0/C1 subluxation, must include the reharmonization of all fascias.

Transbuccal typical radio of KiSS syndrome